
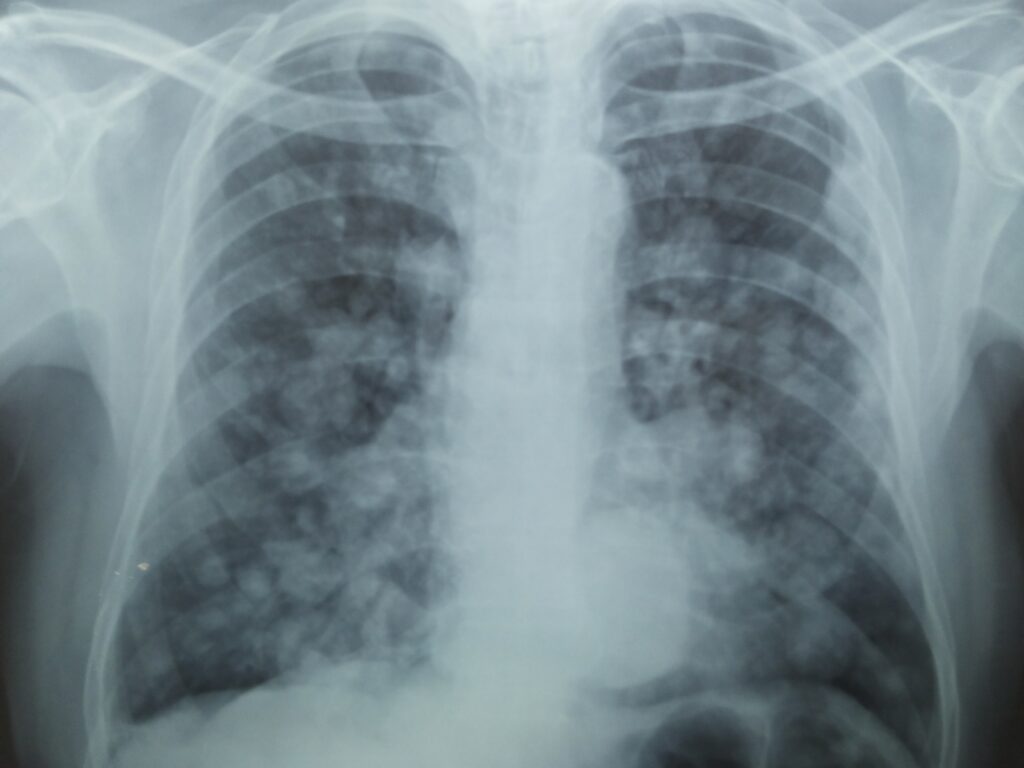
Question: 65 year old male patient with 30 pack years of smoking history presents with history of cough and progressive breathlessness since 2 months. He has been diabetic for nearly 20 years which has been uncontrolled for at least 3 months. He reports significant weight loss and loss of appetite. No history of fever or chest pain or hemoptysis. Describe the findings in this X-ray. What could be the reason(s) for such abnormality?
Answer: Multiple lung nodules in both the lungs. Nodules are of varying sizes and shape. A mass lesion is visible behind the heart shadow in the left lower zone. Most likely they are multiple lung metastases. Retrocardiac shadow can be descending aorta aneurysm or a primary lung malignancy.
Differential diagnosis: Fungal pneumonia.
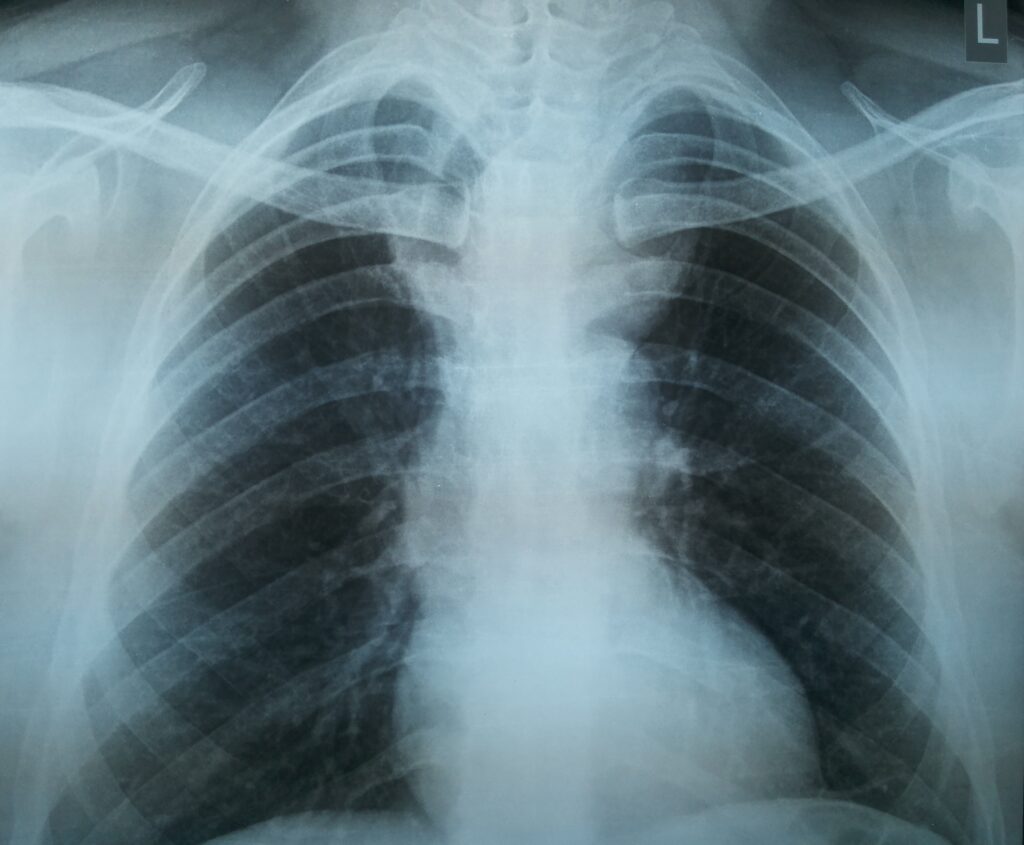
Question: 65 year old male patient presented to medical OPD with 2 months history of exertional breathlessness MRC class 2 and cough with expectoration. No history of fever or chest pain. He has no previous co-morbid illnesses. Non-smoker and works as a agricultural farmer. Describe the abnormalities? What could be the reason for such abnormalities?
Answer: Displacement of right main bronchus, non-visiblity of left main bronchus. Elevation of left hemi-diaphragm (right and left hemi-diaphragms are both at same level, normally left is lower than right) raises a suspicion of partial volume loss in left upper lobe. There is a globular mass lesion visible in the upper central chest area causing displacement of the right main bronchus to more right side.
Possibilities include:
Left side lung cancer with partial left upper lobe volume loss
Mediastinal lymphadenopathy ? TB ? Lymphoma
Retrosternal goiter
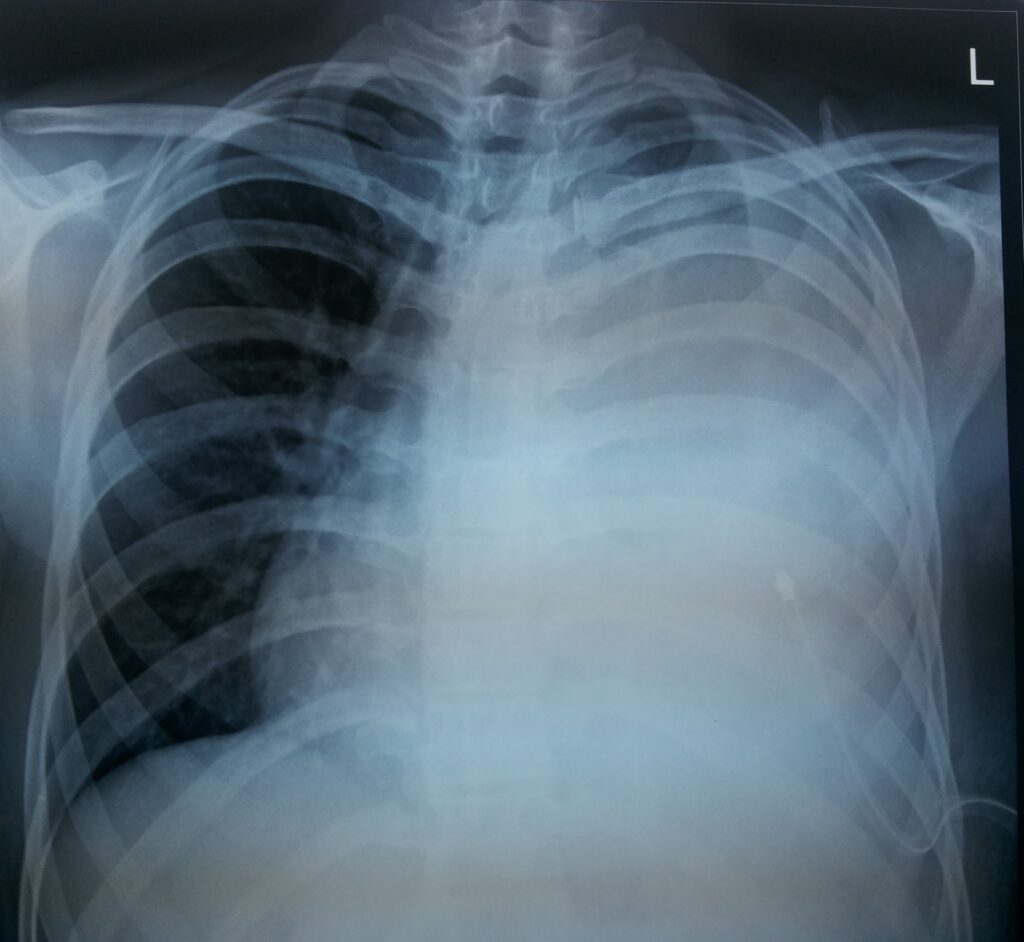
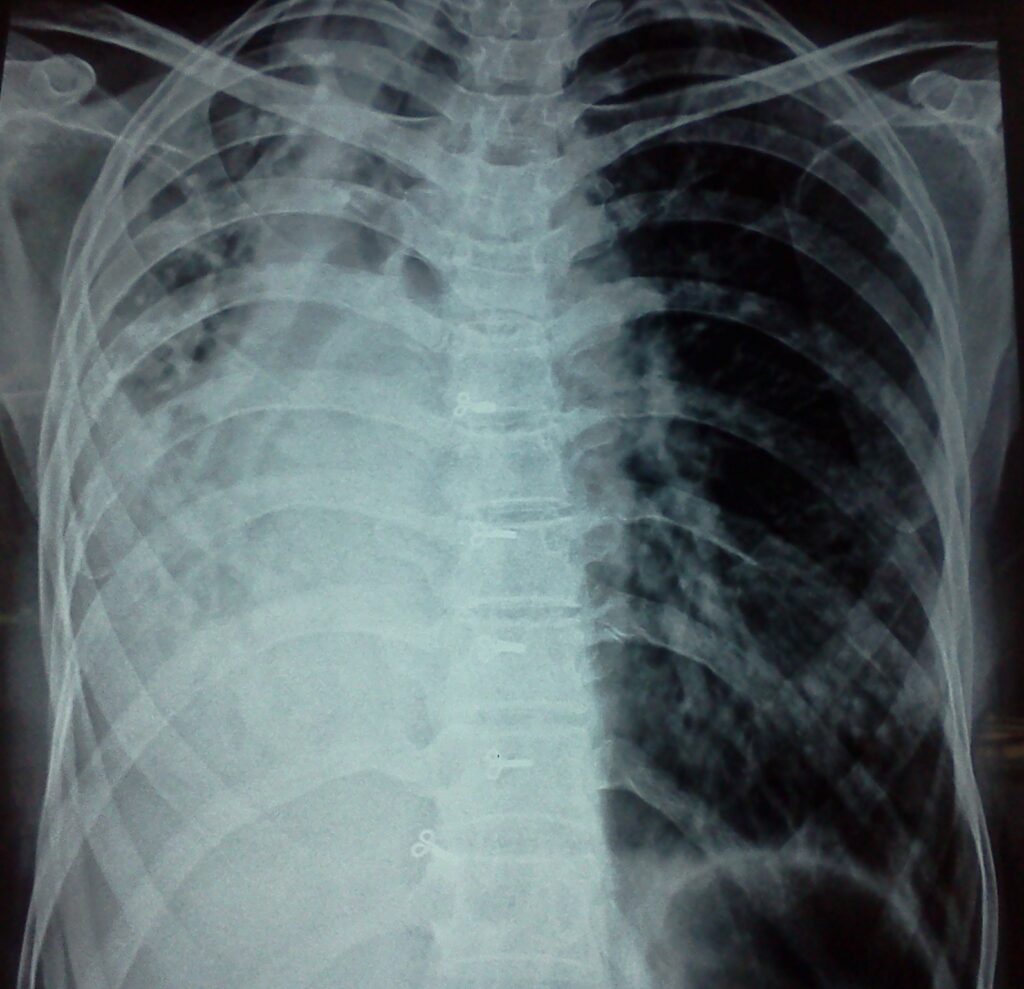
Question: 48 year male patient presented to the emergency department with progressive breathlessness for nearly 1 month which got worse since 3 days. He gives history of losing at least 5 kgs of weight in last 2 months. No history of fever or chest pain. He has no previous co-morbid illnesses. He is a smoker and non-alcoholic.
Describe the abnormalities in the chest x-ray? What could be the possible reasons? How would you like to investigate this patient?
Answer: Hyperdense opacification of the left hemi-thorax. Trachea, right main bronchus and heart is displaced to right side (mediastinal shift). Intercostal drain tube (ICD) is visible inside the left thoracic cavity. ICD inserted to drain the fluid.
Differential diagnosis:
a) Malignant pleural effusion b) Pleural effusion due to Tuberculosis.
Pleural fluid analysis should be performed to check if the fluid is exudate or transudate. Elevated pleural fluid LDH, predominant lymphocytosis and elevated Adenosine deaminase (ADA) levels may indicate TB. Send large volume of Pleural fluid for malignant cells. If fluid analysis is not helpful then perform a CT Chest with I.V contrast and plan for further investigations. Depending on CT findings a bronchoscopy or thoracoscopy with biopsy can be planned next.

Question: 45 year old male patient underwent a routine annual health check up. He reports exertional breathlessness if he does anything strenuous like walking uphill or climbing 1 flight of stairs. There is no history of any co-morbid illnesses. He is an ex-smoker (20 pack years of smoking), stopped smoking 1 year back. He works in a cable manufacturing factory.
Answer: Multiple hyperlucent opacities involving both lungs predominantly in the upper zones. Hyperdense lesion in the right hilar region and increased vascular markings with non-specific cystic areas in left lower zone. These features are in favour of multiple bullous lesions involving both the lungs. The opacity near the right hilar region is the collapsed right lung. The opacity in the left lower zone is compressed left lung due to a large bulla occupying left upper thoracic cavity.
Differential diagnosis:
a) Bilateral bullous lung disease b) COPD- Bullous emphysema

Question: 65 year old Ex-smoker presented to the emergency department with a history of left sided chest pain since 2 days. Chest pain is localized to left precordial region and increasing with movements. No history of cough or fever of breathlessness. He has past history of TB about 20-25 years back for which he took treatment. He is diabetic and hypertensive. ECG is normal and also serum troponin-T levels are normal.
Describe the abnormalities in the chest x-ray? What could be the cause for these abnormalities?
Answer: Hyperdense opacity in the left upper zone. There is displacement of trachea and heart towards the same side (left) and also the volume of left lung is smaller compared to right lung (volume loss mainly left upper zone). Features are in favour of left upper lobe fibrosis. Most probably secondary to Old TB. There is compensatory hyperinflation of the right lung.
Differential diagnosis: other causes of upper lobe fibrosis- radiation, ankylosing spondylitis and Sarcoidosis.
Question: 68 year male farmer presented to the medical out- patient department with history of cough and expectoration for the last 2 years which had increased in the last 3 months with occasional history of coughing up streaks of blood. He also reports exertional breathlessness which is MRC class II. He is an ex-smoker.
Answer: Bilateral cavitary lesions in the upper lobe left>right associated with surrounding hyperdense irregular opacities, elevation of left hemi-diaphragm with tenting. Features are consistent with bilateral upper lobe fibro-cavitary disease with evident features of reduced lung volume on left side. Most common cause for such changes is Tuberculosis. X-ray features such old PTB but in view of symptoms, investigations should be performed to rule out active TB (recurrence of TB).
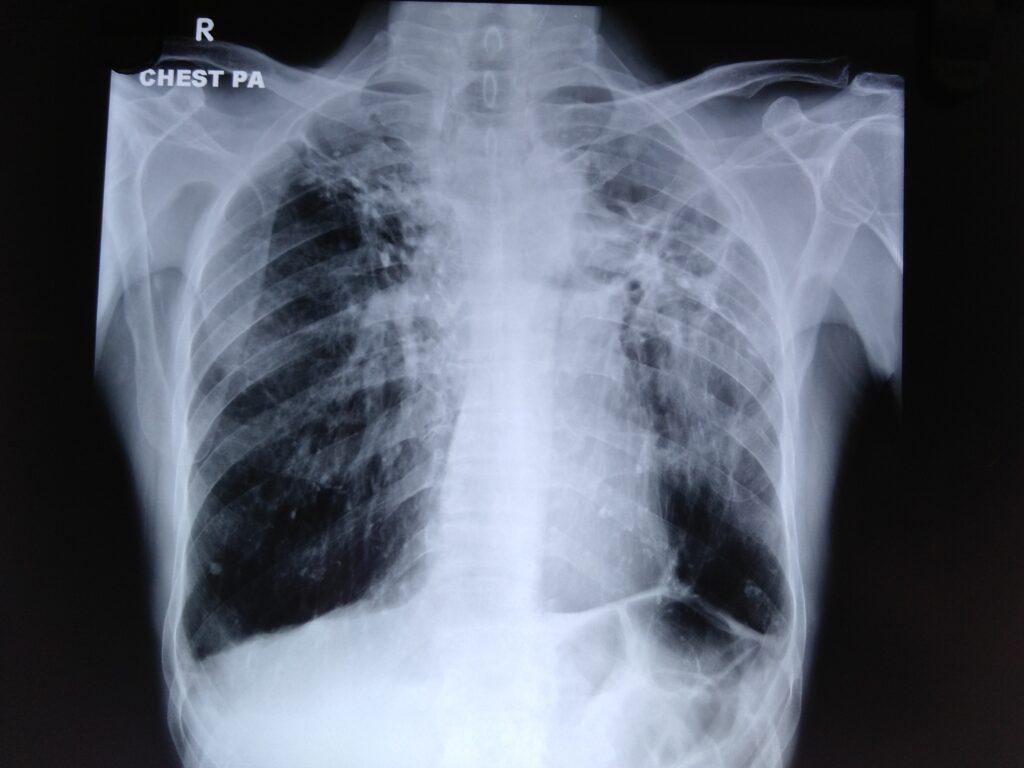
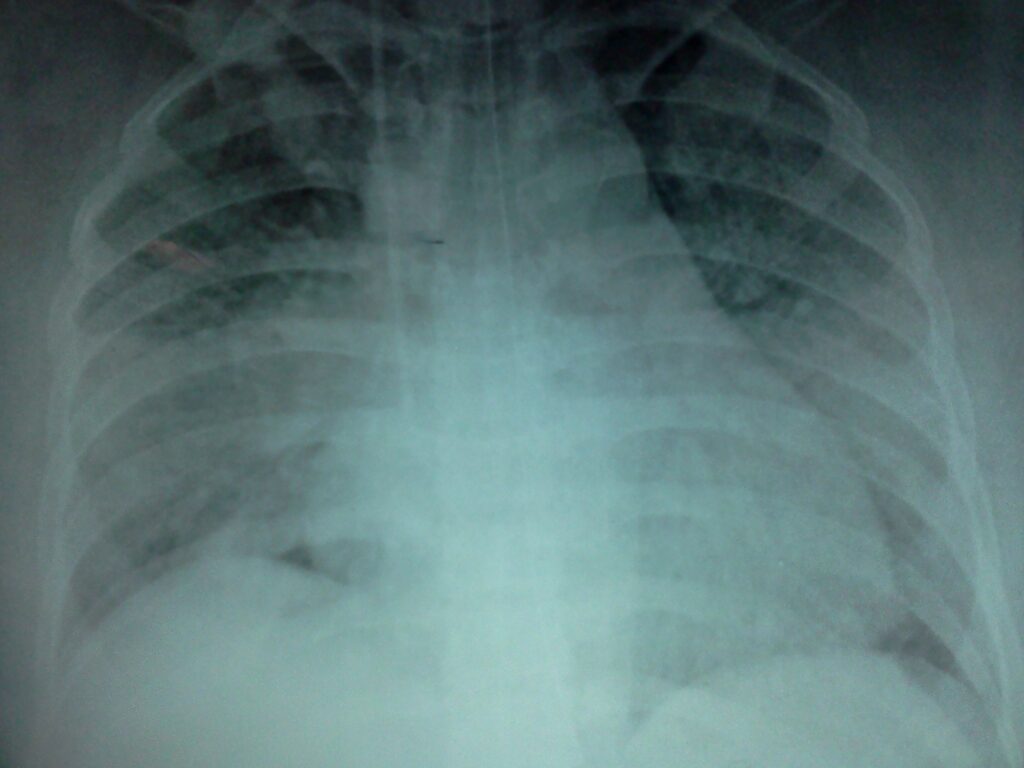
Question: 48 year male school teacher presents with history of fever for 1 week, cough with expectoration of yellowish sputum and occasional blood stained sputum since 3 days. On the day of admission patient complained of breathlessness. On arrival in ER, patient oxygen levels were low (SpO2 78% on room air) and BP was low as well (92/60mmhg). Identify the abnormalities in the chest x-ray? What could be the possible diagnosis or differential diagnosis?
Answer: Bilateral patchy areas of consolidation involving multiple lobes right >left. Features are consistent with bilateral bronchopneumonia. In keeping with clinical picture patient is in severe sepsis.
Differential diagnosis: Diffuse alveolar haemorrhage (pulmonary haemorrhage) and pulmonary oedema. However, presence of fever and yellowish sputum would favour bronchopneumonia as most likely diagnosis.
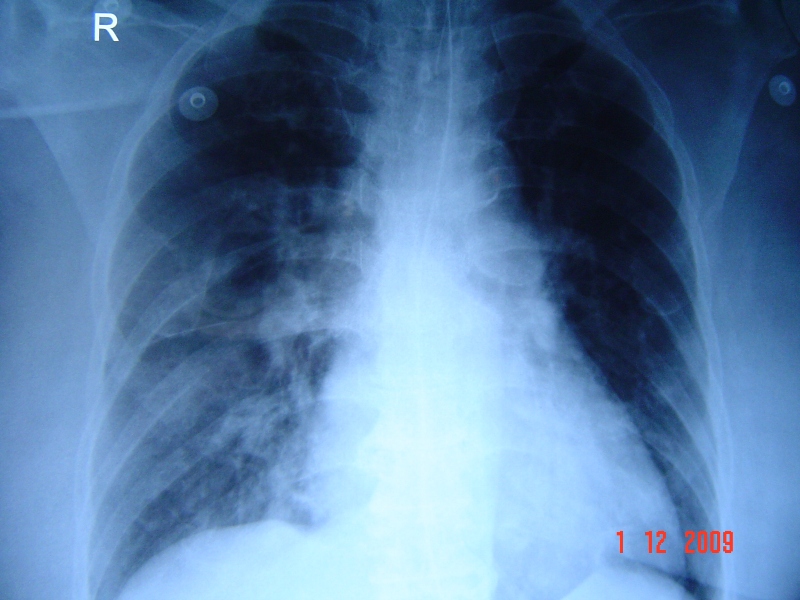
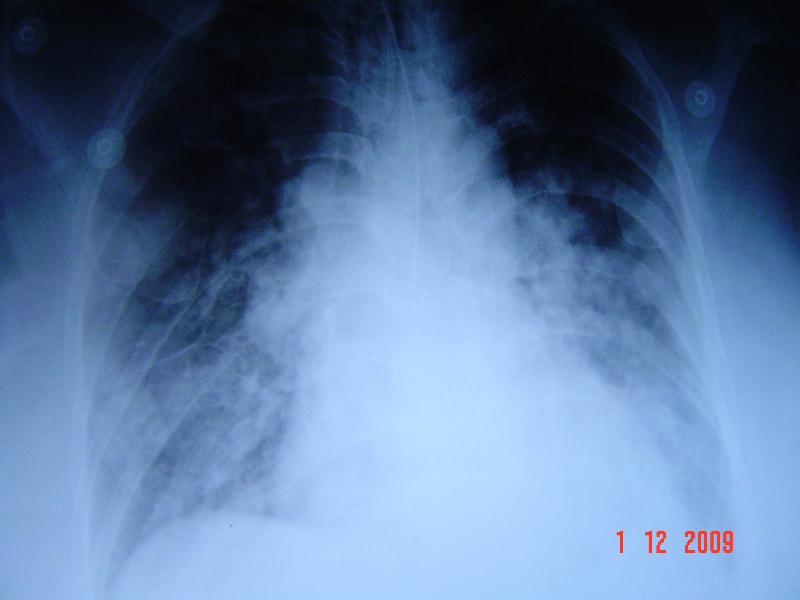
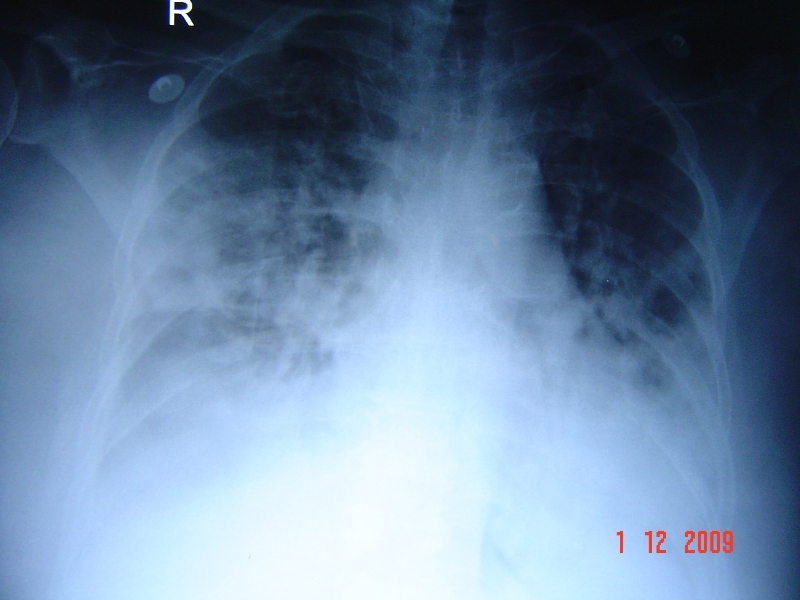
show the X-ray findings from subsequent days. Different appearances of consolidation can be appreciated in these x-rays.
Question: 33 year old male patient with past history of pulmonary TB for which he took treatment for 2 months only 20 years back. He presented to emergency department with history of fever for 5 days and cough with yellowish sputum. Describe the abnormalities in the chest x-ray at the time of admission.
Answer: Hyperdense opacity of right hemi-thorax associated with deviation of trachea to right side and also displacement of heart to right side. Calcified nodules in the right upper zone are seen. Nodular opacities and patchy consolidation in left lower zone. Features are consistent with volume loss of right lung with mediastinal shift to right side.
Right Lung fibrosis secondary to old PTB and active infection in left lower lobe (bacterial or recurrence of TB)
Question: 63 year old male patient presented to emergency department with history of progressive exertional breathlessness MRC class II to class IV over a period of 3 days. Patient gives history of orthopnea and swelling of the feet. Past history includes Ischemic heart disease, Diabetes and Hypertension. Describe the abnormalities in Chest x-ray? What is the most probable diagnosis and differential diagnosis?
Answer: Bilateral diffuse consolidatory opacities involving predominantly peri-hilar areas (left >right). The vertical hyperdense linear opacity in the right side next to the trachea is the opacity due to the central venous catheter inserted into the jugular vein. Radio-opaque linear opacity due to ryles tube is also visible in the centre of the x-ray.
Features are consistent with Pulmonary Edema possibly secondary to ischemic heart disease. Investigations should be performed to rule out a recent myocardial infarction.
Differential diagnosis includes Pulmonary haemorrhage and Bilateral bronchopneumonia.

Question: 58 year old male smoker presented to the medical outpatient department with history of exertional breathlessness MRC class III associated with cough and minimal expectoration since 1 year increased since 2 months. Past history of diabetes and hypertension. 30 pack years of smoking and he works in a steel factory. Describe the findings and most probable diagnosis?
Answer: Hyperinflation of both lungs with the flattening of both domes of diaphragm. Hyperlucency in both the lower lung zones devoid of vascular markings. Tubular thin cardiac opacity in the center.
Features are consistent with Emphysema and bullous lesions in both lower lobes.
